Obesity-Driven Metabolic Disease Clustering: A Weak Signal Reshaping Clinical and Population Health Paradigms
This paper highlights a genuinely under-recognized inflection emerging from the accelerating global obesity epidemic—namely, the systemic clustering of metabolic disorders such as diabetes, cardiovascular diseases, and cancer within expanding obesity populations. Rather than treating these as isolated pathologies, this convergence may catalyze an era of interconnected clinical management and population health strategy transformation over the next two decades.
The mounting prevalence of obesity worldwide is triggering a cascade of interrelated chronic conditions at an unprecedented scale. This clustering creates significant pressure points on existing health systems, regulatory regimes, investment theses, and industry configurations. Current market and policy perspectives tend to silo each disease, overlooking the compound systemic vulnerabilities and new risk dynamics this interplay fosters. Recognizing and preparing for this co-dependent disease ecosystem could markedly influence capital allocation, care delivery models, and disease prevention frameworks.
Signal Identification
This development qualifies as an emerging inflection indicator because it signals a structural shift in how clinical and population health will need to organize and strategize disease management over the next 10–20 years. The plausibility of this shift is high, grounded in robust demographic, epidemiological, and economic trends, though it remains insufficiently recognized in mainstream health policy and industrial planning domains.
The primary sectors exposed include healthcare delivery, pharmaceutical and medical device industries, insurance and risk governance entities, public health institutions, and regulatory bodies overseeing chronic disease management and health promotion.
What Is Changing
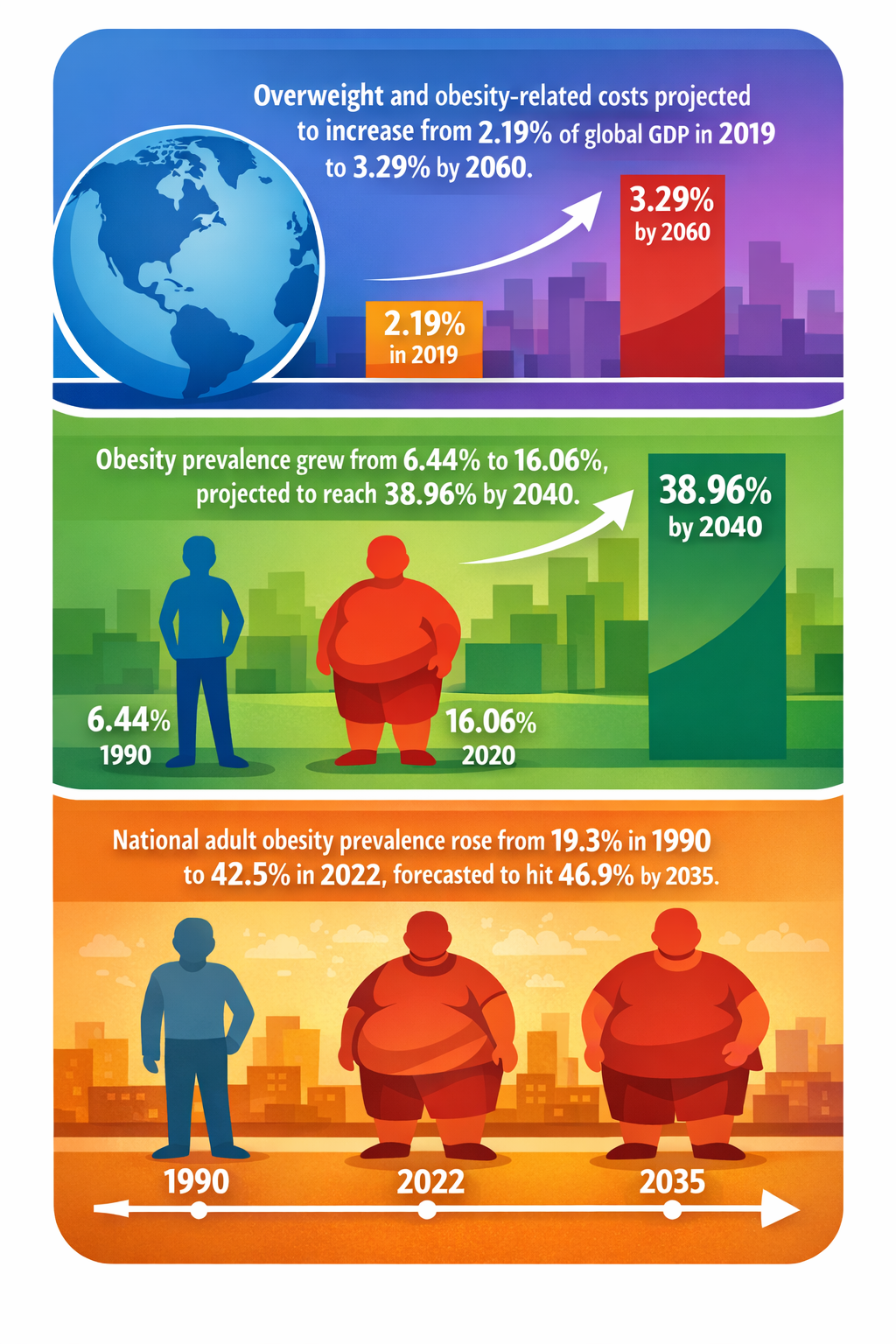
Globally, adult obesity prevalence has nearly doubled in recent decades and is projected to continue rising substantially—reaching 46.9% by 2035 in some countries like the United States (Consultant360 05/06/2023) and surging beyond 38% by 2040 in other regions (PMC 24/04/2023). The accelerating trajectory of obesity prevalence is creating a swelling base population at risk for clustered metabolic disorders.
Diabetes incidence is rising in tandem, with global cases projected to reach 700 million by 2045 (Mediscript 12/01/2024). In developing countries, diabetes cases are forecasted to nearly triple from 84 million in 2000 to 228 million in 2030 (PMC 06/07/2015). This growth not only strains medical management capacities but further blurs disease boundaries, as obesity-related insulin resistance elevates cardiovascular risk profiles.
Concurrently, cancer incidence is expected to increase by 77% by 2050 compared to 2022 baseline levels (Persistence Market Research 04/03/2024). Obesity is a recognized but often underappreciated risk factor contributing to this rise. The linked rise in metabolic inflammation and hormonal disruptions introduces new oncological vulnerabilities linked to obesity and diabetes patient populations.
Economic analyses illustrate the broader societal impacts of obesity interventions—such as a UAE study projecting a potential GDP addition of $51 billion by 2031 through obesity reduction programs (Gulf News 14/08/2022). This reinforces the materiality of obesity-driven disease cluster disruption, beyond the clinical domain, reaching into national economic resilience.
Collectively, these data pieces reveal a systemic pattern: obesity acts as a catalyst transforming discrete chronic conditions into an interlocked metabolic disease cluster, amplifying complexity and costs. This synthesis offers a departure from traditional single-disease centric models toward integrated clinical and population health approaches specifically designed for multimorbid obesity populations.
Disruption Pathway
The growing prevalence of obesity combined with clustered metabolic disorders is creating accelerating demand for poly-centric clinical protocols integrating endocrinology, cardiology, oncology, and nutrition science. This demand could catalyze reconfiguration of healthcare delivery toward multi-specialty integrated care systems, diminishing legacy single-specialty silos.
This integration will be motivated by escalating economic and clinical inefficiencies: fragmented care models increase avoidable hospitalization, compound drug regimens, and exacerbate adverse event rates. Health insurers and governments may accelerate shifts toward value-based care models emphasizing bundled payments for metabolic health cascades.
In regulatory terms, current frameworks that impose siloed disease classifications may increasingly face pressure to overhaul reimbursement, approval pathways, and outcome measures that acknowledge multimorbidity complexity. This could drive standards evolution around multi-indication therapies and diagnostics tools sensitive to overlapping metabolic markers.
Medical technology sectors—exemplified by rapid uptake of diagnostic tools like magnetic resonance imaging (MRI) for tumor staging—may expand investments toward next-generation integrated metabolic health diagnostics, encompassing cardiovascular, diabetic, and oncologic risk stratifications (Persistence Market Research 04/03/2024).
Feedback loops may emerge as improved clustering diagnostics increase detection rates, further amplifying patient complexity and health system burden, which in turn could incentivize preventive and lifestyle interventions scaling. A wildcard could arise if accelerated digital health technology enables real-time, population-scale metabolic health monitoring, enabling predictive analytics that disrupt current reactive care models.
Ultimately, dominant industry and governance models may shift from single-disease verticals to horizontally coordinated metabolic health ecosystems, restructuring pharmaceutical R&D pipelines, insurance risk pools, and public health strategies.
Why This Matters
For capital allocators, understanding this clustering inflection could reorient investment priorities toward integrated care platforms, multi-indication therapies, and advanced diagnostics designed for metabolic multimorbidity.
From a regulatory standpoint, ignoring the clustering effect may perpetuate misaligned incentives and slow adaptive frameworks needed for effective management of complex, interrelated chronic diseases. Industrial players may face disruption unless strategic repositioning encompasses broader metabolic health rather than segmented disease states alone.
Supply chains for pharmaceuticals, diagnostics, and health services will likely require reengineering to handle multi-drug combinations, longer care cycles, and integrated data flows bridging clinical specialties. Governance bodies may confront liability shifts toward coordinated care accountability, necessitating novel policy tools.
Implications
This obesity-driven metabolic clustering may catalyze a paradigmatic shift in population health priorities, introducing integrated disease ecosystems that necessitate new operational, regulatory, and financial models.
The disruption is likely to be structural rather than ephemeral, advancing beyond incremental disease prevalence increases to recast health system architectures and capital flows.
However, this development is not synonymous with digital health hype or genetic precision medicine alone. It specifically anchors in epidemiological realities of metabolic disease systems coalescing and interacting vitally at the population scale.
Alternate interpretations might argue that biomedical breakthroughs in isolated diseases could negate clustering complexities or that lifestyle intervention scalability limits reduce systemic impact; yet current demographic and economic evidence suggests otherwise.
Early Indicators to Monitor
- Larger-scale integrated metabolic multimorbidity studies and surveillance data demonstrating increased co-prevalence trends
- Regulatory agency draft guidelines expanding chronic disease management approval pathways to include multimorbidity endpoints
- Pharmaceutical pipeline shifts toward combination therapies targeting multiple metabolic conditions simultaneously
- Increased capital allocation in integrated care platforms and diagnostic tools designed for metabolic clustering
- Health insurer payment models piloting bundled reimbursement strategies for obesity-linked disease complexes
Disconfirming Signals
- Substantial breakthroughs leading to effective, affordable single-disease cures that decouple disease clustering
- Global public health campaigns reversing obesity trends drastically within the next decade, reducing clustering prevalence
- Persistently fragmented regulatory and reimbursement frameworks limiting integration despite growing disease interconnections
- Failures of integrated care models to demonstrate improved outcomes or cost-effectiveness in metabolic clustering populations
Strategic Questions
- How can capital allocation strategies be adapted to anticipate resource shifts toward integrated metabolic health management rather than siloed disease investments?
- What regulatory frameworks need revision to enable and incentivize the management of complex metabolic disease clusters at scale?
Keywords
Obesity; Metabolic Disease; Multimorbidity; Integrated Care; Population Health; Healthcare Regulation; Diagnostics; Pharmaceutical Investment; Chronic Disease
Bibliography
- Diabetes is a major concern for the developing countries, as its incidence is projected to triplicate from 84 to 228 million cases during 2000-2030 period. PMC. Published 06/07/2015.
- Cancer incidence will rise by 77% by 2050 compared to 2022 levels, with MRI serving as a cornerstone modality for tumour staging and treatment monitoring. Persistence Market Research. Published 04/03/2024.
- The Accelerated intervention could help more than 1.2 million adults in the UAE transition out of obesity by 2031, and prevalence could fall by 15 percentage points and unlock $1.5 billion in cumulative healthcare savings, add $51 billion to GDP in 2031 alone. Gulf News. Published 14/08/2022.
- By 2045, global diabetes prevalence is projected to reach 700 million. Mediscript. Published 12/01/2024.
- The national adult obesity prevalence (BMI ≥ 30) increased from 19.3% in 1990 to 42.5% in 2022 and is forecast to reach 46.9% by 2035. Consultant360. Published 05/06/2023.